 Anatomy/Physiology
Anatomy/PhysiologyIncidence
Here are statistics from the Mayo Clinic (2019) and Neroni, et al. (2014) on the incidence of PSVT:
Anatomy/Physiology
Definition of terms
Anterograde conduction (normal)
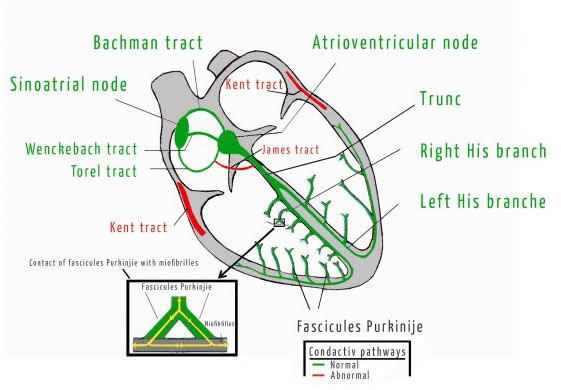
- Cardiac conduction begins in the sinoatrial node (SAN) and spreads through the atria toward the atrioventricular node (AVN) via the internodal tracts.
- The AVN delays the impulse for about 100 milliseconds, then ➤ Bundle of His ➤ (R&L) Bundle branches ➤ Purkinje fibers, causing ventricular depolarization.
Retrograde conduction (abnormal)
- Orthodromic - Because an accessory pathway can conduct impulses faster than the AV node, an impulse may travel through the AV node in the antegrade direction (orthodromic) and reach the ventricle after the impulses from the accessory pathway.
- Antidromic - In addition to causing depolarization in the ventricles, impulses traveling through the AV node can lead to a retrograde movement of the impulse through the accessory pathway (antidromic) into the atria and again through the AV node, completing a circuit. This leads to circus movement tachycardia. Circus movement tachycardias may also occur as a result of impulses traveling through the accessory pathway first and then in a retrograde direction through the AV node (Dowd 2014).
Accessory pathways.
- The cardiac skeleton is a dense, non-conductive, connective tissue layer that electrically insulates atria from ventricles (Saremi 2017).
- Tracts of cardiomyocytes can breach the insulating layer creating a direct connection between an atrium and a ventricle, forming accessory pathways of conduction.
- Kent tract - AV bypass tracts forming direct connections between the atria and ventricles
- Nodoventricular fibers connecting the A-V node to the ventricular myocardium
- James tract - fasciculoventricular connections from the His–Purkinje system to the ventricular myocardium
- A-V nodal bypass tracts, direct communications from the atrium to the His bundle
A study of 189 patients with Wolff-Parkinson-White syndrome, 99 men (52.4%) and 90 female (47.6%), p>0.05, 42.7±14.6 years. Among 189 accessory pathways Left sided accessory pathway was found in 109 patients (57.7%), and right sided accessory pathways had 80 patients (42.3%). 65 patients had septal accessory pathways (34.4%), 84 patients had left free wall sites (44.4%), and 40 patients had right free wall sites (21.2%) (Dung Chu 2017).
An overview description of PSVT includes having a normal conduction system in addition to an accessory pathway. The heartbeat starts in the AVN and down the normal pathway, as usual, but then back up an accessory pathway.
According to Salerno and Seslar (2009) the majority of clinically significant SVT in healthy children is caused by the presence of this accessary electrical connection. This main mechanism underlying SVT is known as reentry. Reentry requires the presence of two electrophysiologically distinct pathways around an insulated core. The diagram in Figure 1 shows these pathways. It is the repetitious cycle and recycling impulse that creates the high pulse rate.
From that description there exists slightly different types of PSVT that are more detailed. PSVT is typically classified in accordance with the anatomic location of the re-entry circuit, also referred to as pathway. Salerno and Seslar (2009) state there are four different classifications with different types of accessory connections that have been identified. The four types are as follows: (Note to self - the ekg descriptions are included in the article)
 The Wolff-Parkinson-White Accessory Connection.
The Wolff-Parkinson-White Accessory Connection.
The Wolff-Parkinson-White (WPW) accessory connection includes abnormal propagation of electrical signals forward (or antegrade) from
the atrium to the ventricle and, in most cases, retrograde
from the ventricle to the atrium. (This is the most common form of PSVT discussed in more detail in the next section.)
The Concealed Accessory Connection.
In this case, the accessory connection between the atrium and ventricle does not disturb electrical signal transmission during normal sinus rhythm. Usually on a routine electrocardiogram (ECG), this accessory connection is “concealed” or not visible. This accessory connection provides abnormal electrical conduction backward or retrograde from the ventricle to the atrium.
Permanent Junctional Reciprocating Tachycardia.
This accessory behaves much the same way as a concealed accessory pathway, except that the rate of transmission of the electrical impulse through the accessory connection is slower than usual. Patients with this form of SVT often have medically refractory arrhythmias that can be quite challenging to manage.
AV nodal re-entrant tachycardia (AVNRT)
In this type of tachycardia, two non-distinct, adjacent conductions pathways exist within or near the AV node. A premature atrial contraction travels anterograde and then backward in a retrograde direction.
Instant Feedback:
Retrograde conduction indicates backward conduction in the heart.
References
Al-Zaiti, S.S., Magdic, K.S. (2016). Paroxysmal Supraventricular Tachycardia: Pathophysiology, Diagnosis, and Management. Crit Care Nurs Clin North Am. 28(3),309-16.
Chu, S. D., Pham, K. Q., & Tran, D. V. (2017, December 4). 12 Lead electrocardiogram algorithm for the localization of accessory pathways using simple parameters in patients with typical Wolff-Parkinson-White syndrome. Interventional Cardiology. https://www.openaccessjournals.com/articles/12-lead-electrocardiogram-algorithm-for-the-localization-of-accessory-pathways-using-simple-parameters-in-patients-with-typical-wo-12260.html.
Dowd, F.J. (2014). Wolff Parkinson White Syndrome. Reference Module in Biomedical Sciences
Neroni, P., Ottonello, G., Manus, D., Atzei, A., Trudu, E., Floris, S. & Fanos, V. (2014). Paroxysmal supraventricular tachycardia: physiopathology and management. J Pediatr Neonat Individual Med. 3(2). e030243. doi: 10.7363/030243.
Salerno, J.C. & Seslar, S.P. (2009). Supraventricular Tachycardia. Arch Pediatr Adolesc Med. 163(3), 268–274. doi:10.1001/archpediatrics.2008.547
https://jamanetwork.com/journals/jamapediatrics/fullarticle/381081
Saremi, F. (2017). Fibrous Skeleton of the Heart: Anatomic Overview and Evaluation of Pathologic Conditions with CT and MR Imaging. Radiographics. https://pubs.rsna.org/doi/10.1148/rg.2017170004
Bashmore, T.M., Granger, C.B., Jackson, K.P., Patel, M.R. (2020). 10-31: PSVT Due to Accessory AV Pathways (Preexcitation Syndromes). AccessMedicine. https://accessmedicine.mhmedical.com/content.aspx?bookid=2683§ionid=225040032.